Documents
Rehab Protocol for a Rotator CuffArthroscopic Shoulder Surgery InstructionsTotal Shoulder Arthroplasty Rehabilitation ProtocolReverse Total Shoulder Arthroplasty Rehabilitation ProtocolArthroscopic Posterior Shoulder Stabilization ProtocolArthroscopic Anterior Stabilization (Bankart) Protocol
Learning Center » Shoulder
Rotator Cuff
Most shoulder pain I see results from rotator cuff problems. Most of the time it’s the result of an inflamed tendon that calms down with conservative care.
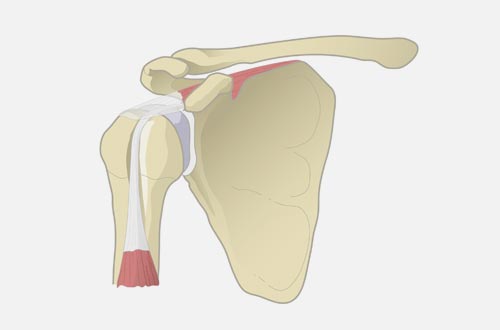
Anatomy
There are four rotator cuff muscles that contribute to strength of the shoulder, particularly with overhead activities. The one that helps with elevating the arm in front of you is the most commonly involved muscle, called the supraspinatus.
There are other structures in the area that often contribute to pain and sometimes occur at the same time. The biceps tendon passes underneath another rotator cuff muscle. There is also a part of the wing bone (scapula) that passes over the top of the rotator cuff like a roof. This “roof” can have projections, called bone spurs, that may cause pain.
Symptoms
An inflamed or torn rotator cuff muscle can be significantly disabling for daily activities. Most people experience pain with overhead reaching, lifting or throwing. Weakness, or a shoulder that tires very quickly, are also common symptoms.
Imaging
X-rays can help reveal arthritis, bone spurs or severe rotator cuff tears. If conservative treatments are ineffective, then magnetic resonance imaging (MRI) can provide a better picture of the muscle, tendon and cartilage to help determine the source of pain and weakness. I now offer in-office ultrasound which is a quick, more convenient, and more cost-effective method of visualizing the rotator cuff during a visit.
Treatments
There are a number of treatment options depending on the specific cause suspected. For the inflamed and painful shoulder I typically start with physical therapy and other helpful forms of treatment (such as ultrasound) to reduce stiffness and regain strength. Oral anti-inflammatory medications and injectable anti-inflammatories (typically a corticosteroid) directly into the space above the rotator cuff muscle, are sometimes necessary and helpful. I use ultrasound guidance for injections in the office to maximize accuracy and comfort during the procedure.
If the rotator cuff is not repairable due to the severity of the injury, some patients are candidates for a procedure called a superior capsular reconstruction. This involves taking a tissue graft and securing it to the ball and socket joint as a substitute for the rotator cuff to help improve pain and mechanics of the shoulder joint.
Surgery
When there is a tear, and symptoms don’t improve with the conservative treatments just discussed, surgery may be appropriate. I perform an arthroscopic surgical repair of the detached muscle. This allows me to see most of the shoulder and assess other structures that may be damaged. Bone spurs can be shaved smooth and the biceps can be repaired (all through the arthroscope) if needed. Potential benefits to the arthroscopic approach include less damage to muscles covering the shoulder and therefore less pain after surgery. Scarring is less obvious since I usually perform this through four small 8-10mm wounds.
Recovery
Surgery is performed as an outpatient procedure. Most patients head home within an hour of completion. A special sling to cushion and protect the repaired muscle is used the first month. During this first month, the patient performs range of motion exercises, under the guidance of a physical therapist, to help reduce stiffness. During the second month, strengthening exercise is introduced gradually and the sling is discontinued. After four months patients can engage in gentle, sport-specific drills. At six months it’s possible to return to sports.

SLAP tear
This is usually caused by either a traction or compression injury to the shoulder. This condition typically causes a deep “toothache” type of shoulder pain. The “SL” stands for superior labrum, where the biceps tendon attaches above the shoulder socket. Typically there is pain with outstretched arm activities. The diagnosis may be made clinically, and isn’t always visible on MRI examinations.
If therapy treatments are unsuccessful and pain limits function, shoulder arthroscopy is an option. During surgery, the two main options involve cutting the tendon free, or cutting and repairing it to another location (called a ‘tenodesis’). Cutting the tendon free creates a higher risk of a biceps prominence in the arm, along with some cramping. If I can repair it, I typically tell the patient to limit elbow bending for six weeks, and no overhead strength activities for four to six months.
Arthritis
Shoulder degenerative arthritis typically causes pain and/or catching and clicking of the shoulder. Symptoms are caused by loss of the cartilage surface on the ball and socket joint, along with loose bone fragments that may float around. Anti-inflammatory medications may be helpful (along with intermittent steroid injections).
If these treatments are ineffective, shoulder replacement is an option. If rotator cuff muscles around the shoulder are torn, sometimes a different type of replacement must be done, called a ‘reverse’ shoulder replacement. I usually restrict my shoulder replacement patients to no more than 10 to 15 pounds lifting with that arm for the rest of their lives. This helps reduce the chance of loosening and further surgery down the road.
Before surgery, a three-dimensional map of the shoulder socket is created with imaging that allows the surgeon to plan out the precise placement of the implants before the day of surgery. During the surgery itself, the computer navigation guides are used to position the implants more accurately.
Biceps Tendonitis
Pain in the front of the shoulder can result from an inflamed biceps tendon where it enters the shoulder joint. There is a groove the biceps tendon lives in and biceps tendonitis usually involves tenderness in that area. It can be worsened with outstretched arm activities (due to tension on the biceps tendon). Physical therapy with ultrasound treatments and anti-inflammatory medications may prove helpful. Sometimes I inject a steroid into the sheath around the biceps to relieve symptoms.
Shoulder Dislocation
During a direct injury to the shoulder, the ball and socket can sometimes become separated. If the ball stays out of the joint, this dislocation sometimes has to be put back into place in the hospital with anesthesia. In younger persons, there is a much higher chance that there will be another dislocation in the future. Non-surgical rehabilitation involves functional therapy with a sling initially, and a brace for sport. If there are recurrent dislocations, or the patient is at high risk for re-injuring (due to sports participation), then surgery is considered. I perform an arthroscopic repair of the torn structures, and follow with six weeks in a sling followed by gradual sport-specific rehab. It is a minimum of six months before returning to sports after surgery.
Documents
Rehab Protocol for a Rotator CuffArthroscopic Shoulder Surgery InstructionsTotal Shoulder Arthroplasty Rehabilitation ProtocolReverse Total Shoulder Arthroplasty Rehabilitation ProtocolArthroscopic Posterior Shoulder Stabilization ProtocolArthroscopic Anterior Stabilization (Bankart) Protocol